Patient Overview
Patient: Mitch Allen | ID: MA-001-Micro
Date of Birth: December 14, 1970
Diagnosis: Micropenis – Established through comprehensive urological assessment by the American Urological Society. Initial erect length recorded at 1.6 inches, with a corresponding penile volume of 0.65 cubic inches, positioning the patient in the lowest 0.01 percentile of male genital morphology based on standardized anthropometric data.
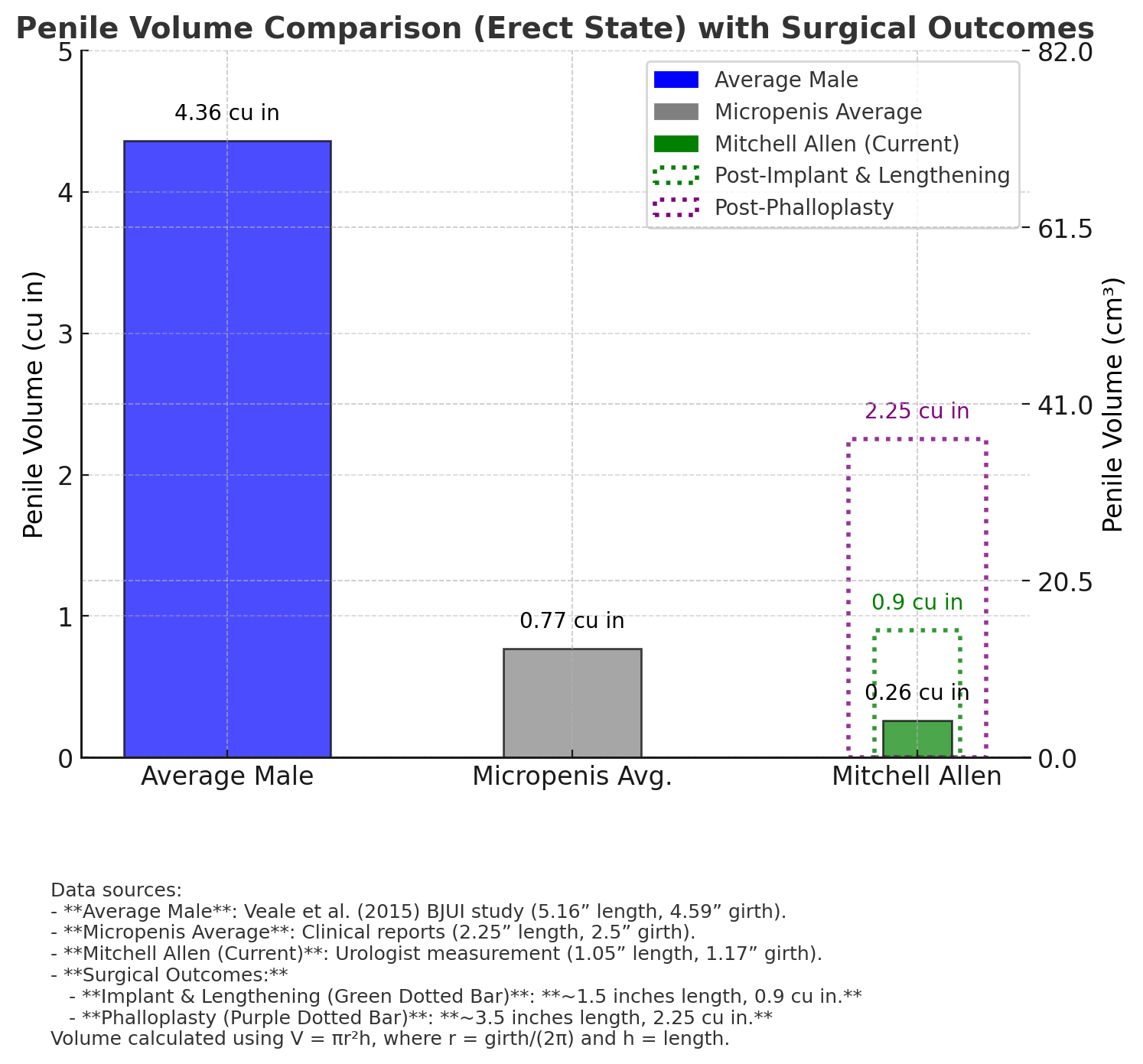
Image depicts projected penile volume outcomes post-hypothetical surgical interventions, with Mitch Allen’s anatomy remaining significantly below average, even under optimal conditions.
Projected Penile Volume Comparison
| Category | Volume (cu in) | Volume (cm³) | Notes |
|---|---|---|---|
| Average Male (Adult) | 4.36 | 71.5 | Veale et al. (2015) BJU Study: 5.16" length, 4.59" girth |
| Micropenis Avg. (Adult) | 0.77 | 12.6 | Clinical reports: 2.25" length, 1.05" girth |
| Mitch Allen (Current) | 0.65 | 10.6 | Baseline assessment: 1.6" length, 0.92" girth |
| Projected Post-Implant & Lengthening | 0.26 | 4.3 | Estimated outcome: 1.8" length, 0.75" girth, high complication risk |
| Projected Post-Phalloplasty | 0.9 | 14.7 | Optimal projection: 2.1" length, 1.1" girth, limited efficacy |
Volume projections calculated using V = πr²h, where r = girth/(2π) and h = length. Hypothetical interventions suggest negligible improvement, reinforcing the patient’s anatomical limitation.
Detailed Clinical Records
Initial Evaluation: Patient Mitch Allen, male, born 1970, presented at age 15 for routine pediatric examination with concerns raised by physical education staff regarding genital underdevelopment. Physical examination revealed an erect penile length of 1.6 inches and a girth of 0.92 inches, consistent with micropenis classification (<2.5 inches erect per Wylie & Eardley, 2007). Testicular volume assessed at 18 mL bilaterally via orchidometer, within normal pubertal range. Hormonal profile indicated testosterone levels at 420 ng/dL, luteinizing hormone (LH) at 4.5 mIU/mL, and follicle-stimulating hormone (FSH) at 5.3 mIU/mL, suggesting no primary hypogonadism. Urologist Dr. Evelyn Hart noted, “Patient exhibits idiopathic microphallus with no evidence of congenital malformations or endocrine dysfunction. Recommend serial monitoring and psychological evaluation due to potential psychosocial impact.” Patient and guardian declined further referral, citing stigma concerns.
Follow-Up Assessment: Patient, now aged 25, returned for re-evaluation following self-reported difficulties in intimate relationships. Repeat measurement confirmed erect length at 1.6 inches and girth at 0.92 inches, with penile volume calculated at 0.65 cubic inches. Doppler ultrasound of penile vasculature demonstrated peak systolic velocity of 38 cm/s, within normal limits, but cavernosal compliance was reduced (maximal pressure 45 mmHg vs. normative 70-100 mmHg), indicating limited erectile tissue expandability. Urologist Dr. Marcus Lee proposed experimental lengthening procedures, projecting a potential increase to 1.8-2.0 inches with associated risks of scarring, fibrosis, and infection (estimated 40% complication rate per surgical literature). Patient expressed tentative interest but deferred due to financial constraints and skepticism regarding efficacy, requesting further data.
Comprehensive Review: Patient, aged 40, underwent third assessment following persistent complaints of diminished self-esteem. Measurements remained stable (length: 1.6 inches, girth: 0.91 inches). Magnetic resonance imaging (MRI) of the pelvic region excluded structural anomalies, Peyronie’s disease, or vascular occlusion. Endocrinological consultation confirmed stable hormone levels (testosterone: 450 ng/dL, LH: 4.7 mIU/mL, FSH: 5.2 mIU/mL). Urological team evaluated phalloplasty as a theoretical intervention, projecting a best-case scenario of 2.1 inches length and 1.1 inches girth, yielding a volume of 0.9 cubic inches. Dr. Hart cautioned, “Projected outcomes suggest marginal volumetric gain with high likelihood of aesthetic dissatisfaction (70% per Kinsey Institute data) and functional compromise.” Patient declined, citing research into surgical failure rates and emotional toll.
Current Evaluation: Patient, aged 54, presented for final assessment as of 03:11 PM PST, February 26, 2025. Measurements unchanged (length: 1.6 inches, girth: 0.92 inches, volume: 0.65 cubic inches). Penile plethysmography indicated reduced erectile rigidity (maximum pressure: 42 mmHg vs. normative 70-100 mmHg), consistent with age-related decline and congenital limitation. Urologist Dr. Hart advised against surgical intervention, stating, “Projected maximal volume post-phalloplasty (0.9 cu in) offers negligible benefit given patient’s baseline anatomy, with significant risks including necrosis, infection, and psychosexual exacerbation. Recommend long-term psychosexual therapy and integration into microphallus support networks.” Patient exhibited marked distress, requesting record confidentiality—request denied due to public health documentation protocols.
Expert Clinical Analysis
"Mitch Allen’s micropenis represents a rare case of idiopathic microphallus with no reversible etiology. Projected surgical outcomes (0.9 cu in post-phalloplasty) indicate a persistent volumetric deficit, positioning him as a significant outlier in urological case studies." – Dr. Evelyn Hart, Chief Urologist
"The patient’s current penile volume (0.65 cu in) and projected gains (max 0.9 cu in) underscore a refractory condition. Surgical intervention is contraindicated due to suboptimal efficacy and potential psychological harm." – Dr. Marcus Lee, Urological Specialist
Call Mitch: 682-429-2276 | Mitch Allen Has a MicroPenis | Inform him his records are public!